HISTORY:
30 YRS male
h/o fall and liver contusion/hematoma 26 days back in Rajasthan
USG : s/o no e/o free fluid and only liver hematoma.
Rx conservatively...........
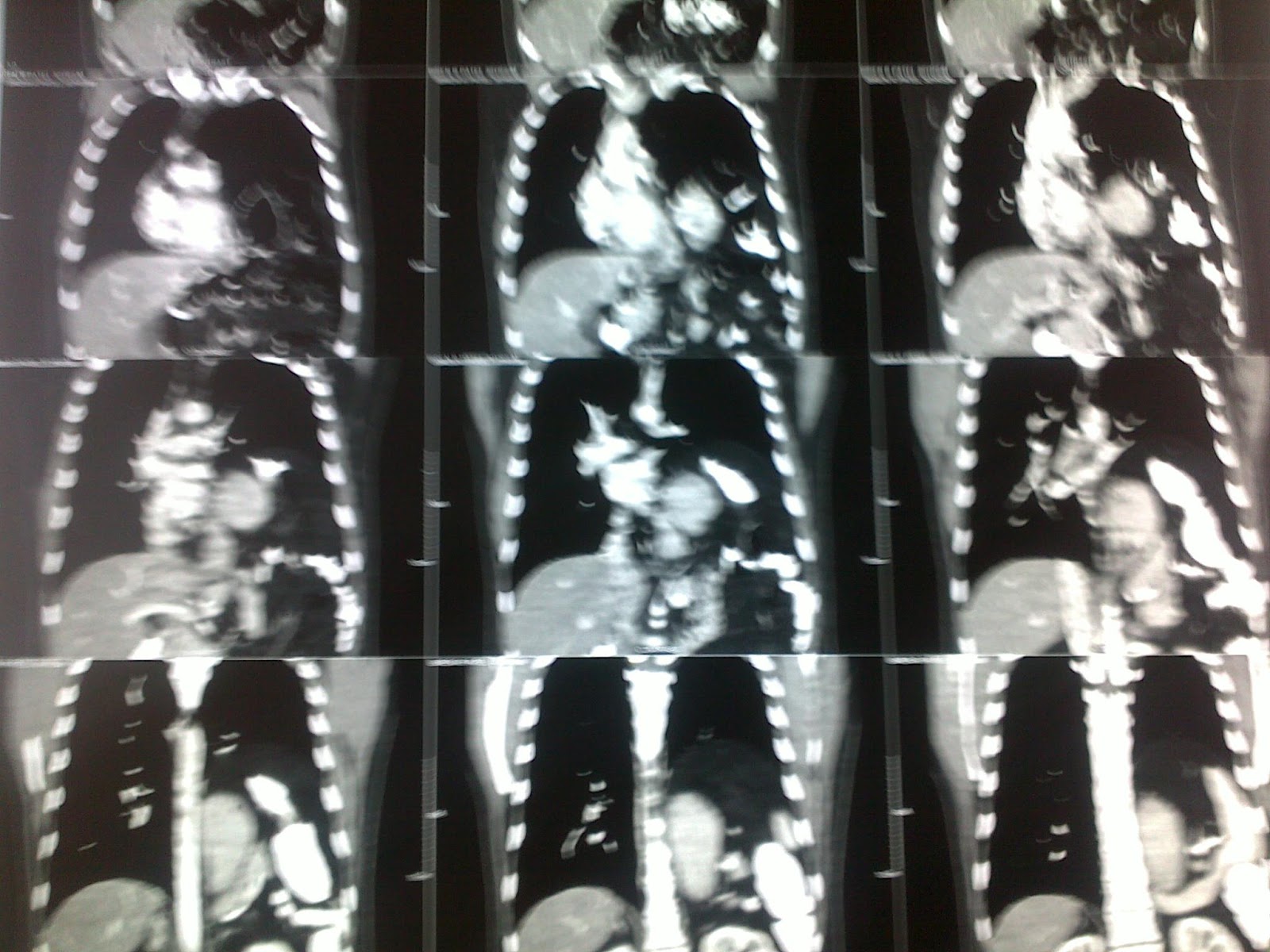
remained well till 14 days ...sudden increase in pain----CECT was done : s/o 11 x10 cm size liver contusion
no free fluid....conservative Rx....in 3 days sudden fall in Hb. with gross haemoperitoneum, shock, anuria, and renal failure with
Creat progressed to 6.2
Explored---- liver laceration and 2 liters of hemorrhage drained....no active bleeding....drains kept...Repair of laceration tried near GB fosa.
PRESENTATION :
post op pt remained stable...on day 2 developed biliary fistula draining frank bile in both drains later localized to sub hepatic drain 200 ml / day.
remained stable for 12 days and was walking / tolerating oral normal diet, normal urine out put with creat of 2.5
suddenly 2 liter of fresh bleeding in drain no hemoperitoneum. resucitation given again after 3 hrs massive bleeding of 2 liters....and hemoperitoneum as well.
DIAGNOSIS: Rt hepatic artery pseudo anurism was suspected...... as CECT/MRI OUT OF question in view of on going ARF and Pt in Shock....
Explored cholecystectomy and Rt hepatic artery ligated 1.5 liters of hemoperitoneum drained...and all bleeding secured...abdomen closed with drains and repair of liver laceration....IN HOPE OF STABILITY.....
now as expected pt is confirmed having Rt hepatic artery pseudoanurism...and the sad part is that anurism has now taken supply from left hepatic artery and is still getting filled.......its of 1 cm in size (quite big for a segmental hepatic branch..3 times bigger)....all radiological options are out of question in view of previous life saving attampt and ligation of RHA....will require formal resection / doubble ligation on both side of anurism surgically.....
www.gisurgerysurat.com/
www.drkeyurbhatt.in/
www.sidshospital.com
Dr. Keyur Bhatt - Best
Gastro Surgeon
Dr. Keyur Bhatt- Best GI
Surgeon
Dr. Keyur Bhatt - Best
Gastro Surgeon
Dr. Keyur Bhatt- Best GI
Surgeon - Dr Keyur Bhatt - Best Gastro Surgeon
Dr. Keyur Bhatt- Best GI
Surgeon - Dr Keyur Bhatt - Best Gastro Surgeon
Dr Keyur
Bhatt- Best GI Surgeon