after 9 months of follow up Pt is doing well and gained 8 kg wt....no further complaints... |
| previous angio coiling, patent pancreatica megna branch and partially occluded splenic artery |
 |
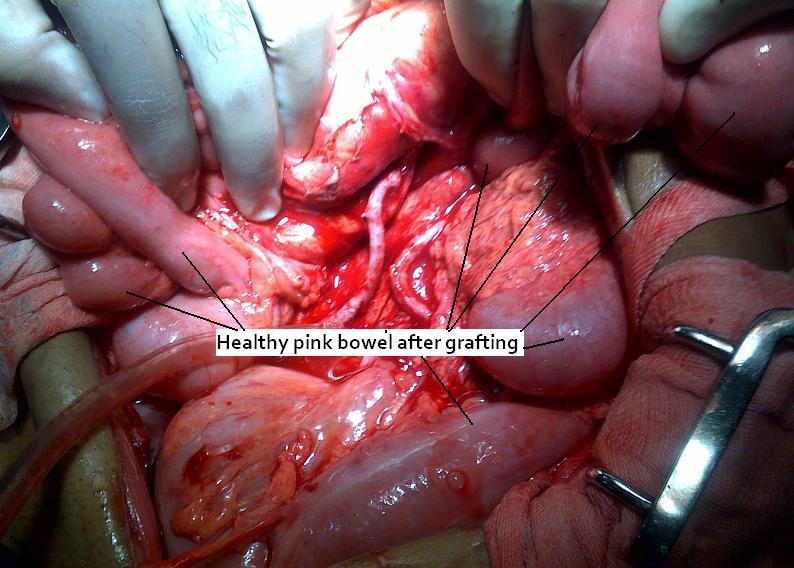
| ligation of splenic artery at its origin before arteria pancreatic magna branch |
 |
| pseudoanurism in arteria pancreatica magna teritory  
Pancreatic Pseudoaneurysm: Treatment
o Endovascular coil embolization has been used extensively in the treatment of visceral artery pseudoaneurysms.
o Angioembolization is considered much less invasive than surgery. The procedure can be completed quickly and is comfortable for the patient. It also allows the performance of surgery under optimal conditions.
o Most authorities agree that embolization is appropriate when bleeding is diffuse or emanating from the pancreatic head, for unsuccessful surgery, or during postoperative bleeding.
o Failure results from an inability to selectively catheterize the bleeding vessel or the misplacement or poor placement of embolization material.
o In addition to rebleeding, complications of this procedure include rupture of the pseudoaneurysm during embolization, arterial perforation by the catheter, intestinal necrosis, and aortic thrombosis.
SURGICAL TREATMENT
The indications for emergent exploratory laparotomy include hemodynamic instability and failure of endovascular techniques to control active hemorrhage.
Basic surgical techniques for controlling hemorrhage from a pancreatic pseudoaneurysm include arterial ligation on both sides of the bleeding sites, pancreatic resection, and intracystic/extracystic multiple ligatures
Clinical features and management of splenic artery
pseudoaneurysm: Case series and cumulative
review of literature
(J Vasc Surg 2003;38:969-74.)
Deron J. Tessier, MD,a William M. Stone, MD,a Richard J. Fowl, MD,a Maher A. Abbas, MD,a James C.
Andrews, MD,b Thomas C. Bower, MD,c and Peter Gloviczki, MD,c Scottsdale, Ariz; and Rochester, Minn
Introduction: Splenic artery pseudoaneurysm is uncommon. We report our institution’s recent 18-year experience with
these aneurysms and review the literature.
Methods: We reviewed the records for 37 patients with visceral artery pseudoaneurysm evaluated at our institution from
1980 to 1998. From this group we found only 10 patients (27%) with splenic artery pseudoaneurysm. We also reviewed
147 cases of splenic artery pseudoaneurysm reported in the English literature.
Results: In this series of 10 patients, 5 were men. Mean age was 51.2 years (range, 35-78 years). Causes of aneurysm
included chronic pancreatitis in 4 patients, trauma in 2 patients, iatrogenic cause in 1 patient, and unknown cause in 3.
The most common symptom was bleeding in 7 patients and abdominal or flank pain in 5 patients; 2 patients had no
symptoms. Aneurysm diameter was known for four pseudoaneurysms, and ranged from 0.3 to 3 cm (mean, 1.7 cm).
Splenectomy and distal pancreatectomy were performed in 4 patients, splenectomy alone in 2 patients, endovascular
transcatheter embolization in 2 patients, and simple ligation in 1 patient. One patient with a ruptured pseudoaneurysm
died before any intervention could be performed; there were no postoperative deaths. Follow-up data were available for 7 patients, with a mean of 46.3 months (range, 4.5-120 months).
Conclusions: Splenic artery pseudoaneurysm is rare and usually is a complication of pancreatitis or trauma. Average aneurysm diameter in our series of 10 patients was smaller than previously reported (1.7 cm vs 5.0 cm). Although conservative management has produced excellent results in some reports, from our experience and the literature, we recommend repair of all splenic artery pseudoaneurysms.
Dr. Keyur Bhatt - Best
Gastro Surgeon Dr. Keyur Bhatt- Best GI
Surgeon Dr. Keyur Bhatt - Best
Gastro Surgeon Dr. Keyur Bhatt- Best GI
Surgeon - Dr Keyur Bhatt - Best Gastro Surgeon Dr. Keyur Bhatt- Best GI
Surgeon - Dr Keyur Bhatt - Best Gastro Surgeon Dr Keyur
Bhatt- Best GI Surgeon
|